What a day! We did seven surgeries today including repairing a traumatized iris prolapsed for a young four years old boy. We did surgery until late, even after the big generator has stopped, and the big light is out. We use the iPhone flashlight often.
By the grace of God, the team arrives safely at Redemption Hospital through the horrendous morning traffic and the crazy maneuvers of large sixteen wheelers tow truck near the entrance to the Monrovia Freeport on Somalia road. When a truck decides to do a U-turn on Somalia road, traffic on both ways comes to a standstill waiting for the large truck to finish its moves. At the midpoint of the U-turn, the truck would just cut off traffic completely going both ways and slowly makes it back and forth maneuvers until it is lined up to go in the driver desired direction. All the while, we have cars and tut-tuts and other vehicles mixed in with pedestrians peddling the things they are selling, either carrying them on their heads or pushing their coconuts and drinking water in plastic bags in wheel barrels. It is a dizzying scene and I wonder how many accidents happen a day. But amazingly, we actually have not witnessed one accident since we arrived and we have not even seen an ambulance here.
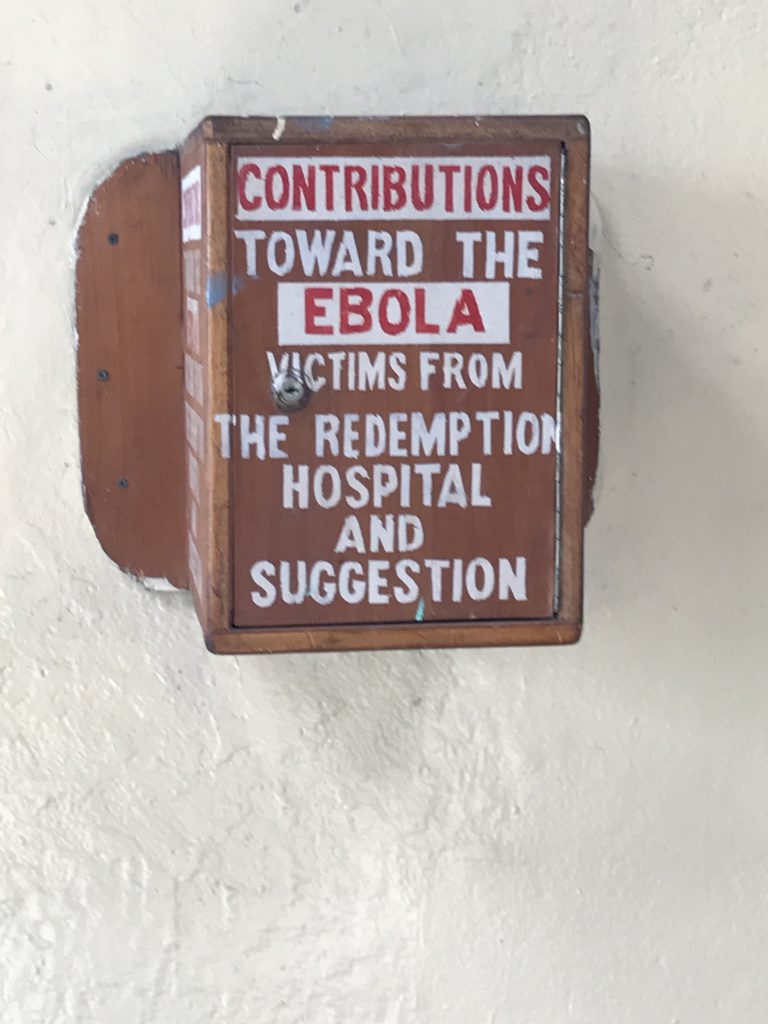
As we enter the hospital, we are reminded of the tough time in Liberia during the Ebola outbreak:
This morning’s waiting room scene. Always very crowded with a lot of people waiting.


And the hallway is equally full

Some of them have traveled a great distance to come here to seek help.
Here is a blind patient being guided by another adult.

At times, there is chaos in the waiting area. Somebody would yell out to our optometrist:
“Dr. Major, there’s somebody who just dropped outside in the waiting hallway.”
“What do you mean dropped?”
“We don’t know, they just drop on the floor.”
“Give them CPR. Maybe they are hungry. Or thirsty. Give them something to eat or drink.”
“We don’t know CPR.”
“It’s a hospital for crying out loud. Somebody do something. I am an optometrist here. Get ER or something.”
Poor Dr. Major. She is such hard working optometrist! She has screened hundreds of patients the past three days. We brought back three thousand five hundred pairs of glasses. I am sure by the end of the mission, she will have all those glasses given out.
The “dropped” patient was taken care of. But all day long, just one thing after another in the screening area. Ed says it is stressful driving from the hotel to the hospital, it is chaotic in the waiting area. The only time he is relaxed is when he is doing surgery! Quiet and calm!
The long line of patients is waiting for the doctor to arrive.
We head straight to the operating room trying to have an early start for the day. No dilly-dallying. Notice the posted Generator hour.
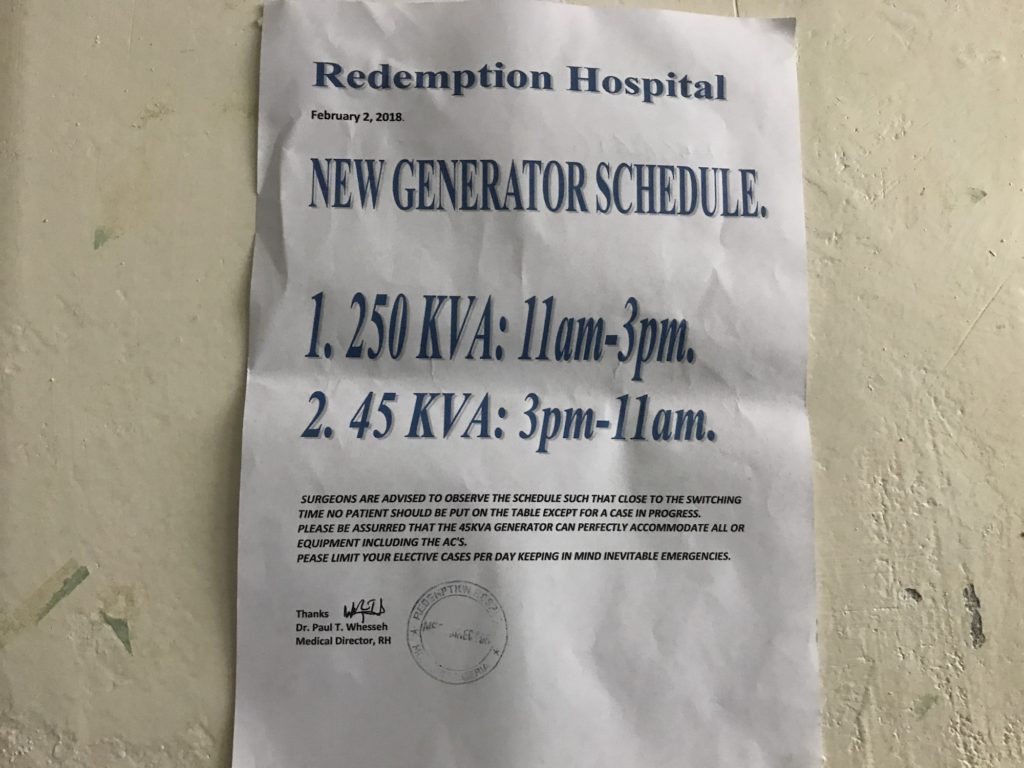
It is now only 9 AM. We are starting to sweat but no luck for air conditioning until the big generator comes online. We have to wait until 11 AM. And we also have to deal with the dim light condition in the operating room as the big overhead operating light can only be used when the big generator is on.
This morning we have our first post-op patient. We did surgery on Lucy yesterday and this morning we took out her bandage. She is so happy she can see again. She thanks us profusely and she is very happy with her newfound eyesight.

Her post-op instructions are as follow:
No bending her head down
No eating tough food that she yanks roughly side to side
Not sleeping on the side of operation
Wear shield one week at night
No strong soap on face
No bucket on head
No holding or carrying children in their arms as children might hit the surgery site
(Notice the instruction to the local woman: no carrying bucket on the head. Imagine giving that post-op instruction to a woman in the US!)
Second post-op patient:

Then we head over to the pediatric ward for pre-op for the four years old boy we are going to operate on today. He is in very good spirit and eager to have the treatment done. He is such good trooper!

A scale in the pediatric department.
 l
l
We are now ready to start the new day. As we begin to set up, we notice that the microscope lost the eyepiece.
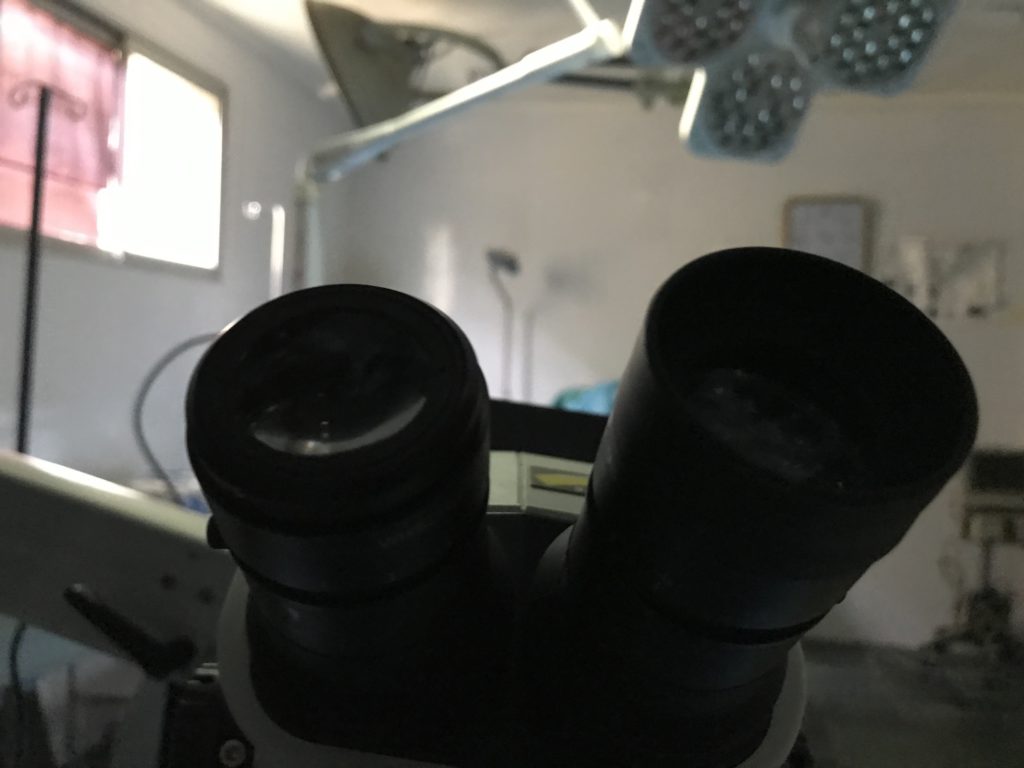
It’s a mad dash all around the OR looking for the eyepiece.The garbage can is turned inside out. We can’t wait too long and lose time so Ed says he will work with the microscope as it is!
The good news today: Ed gets an upgrade! A better chair to sit today. And here is his better chair:

As you can see, the chair looks very stable but it does not have any wheels, so if Ed needs to move forward or backward or change his sitting position slightly, he has to move his body into position and asks me to place the chair under him so he can sit himself down. We lovingly say to each other that gives me something to do and I am now officially his chair manager.
While all the search is going on in the OR for the missing eyepiece to the microscope, the first patient is singing and praying for both doctor and patient and even for the doctor’s wife!

Today we have extra help with a retired nurse Rita and the senior nurse Neda as Neda had a one-afternoon training yesterday to assist Dr. Kondrot.
After we finish with this patient, we move to operate on a four years old boy to repair a traumatic Iris prolapsed injury when a stick punctured his eye. When the stick got pulled out the iris is damaged and there is a risk of infection and later could lead to loss of the eye if not repaired in time.
Baby is wheeled in with a balloon.


Anesthetist starts the procedure and soon the baby is knocked out.

Race against time as there is a risk of the big generator being shut off

And done just in time before the big generator shuts off!

Good job Dr. Kondrot! He did it in time!
The third patient is a one eye patient but fully functioning. After Dr. Kondrot checks her out, he says she is not a candidate as she is driving, reading and fully functioning even though she has a cataract. I try to explain to her it is not a good idea to do the surgery today. She should wait. She started crying saying “doctor nothing can be done for me?”. I say “no it is not necessary to do the operation today, may later in the future when her vision is worse then we can do it but now she is functioning so why do it? She has a fully functioning life she should wait. It took a while to explain to her but she still insists on having surgery done. It is time to bring in the big guns, she needs a little bit of Liberian tough love so I take her hands and tell her to follow me. I take her over to our optometrist who is Liberian and the local optometrist who is of course also Liberian. I explain to them to the situation and they both agree with me and told me “don’t worry we will talk to her”. So I left her with the very able hands of the two Liberian doctors.
It is now 2 PM and we have not had lunch. Ed has a muffin before we start the next case. We will eat after we finish this next case. Was it a gluten-free muffin? I doubt it. But hunger is the best sauce. It is the finest six days old blueberry muffin from our flight over that I kept in my backpack that suddenly became very handy in case of an emergency!
And we got lucky, we found some breakfast food laying around! Yes, we need the energy boost!
And the power is out!
The third patient today is a buffalo bill fan who went to America and now is back in Liberia. Surgery goes smoothly.

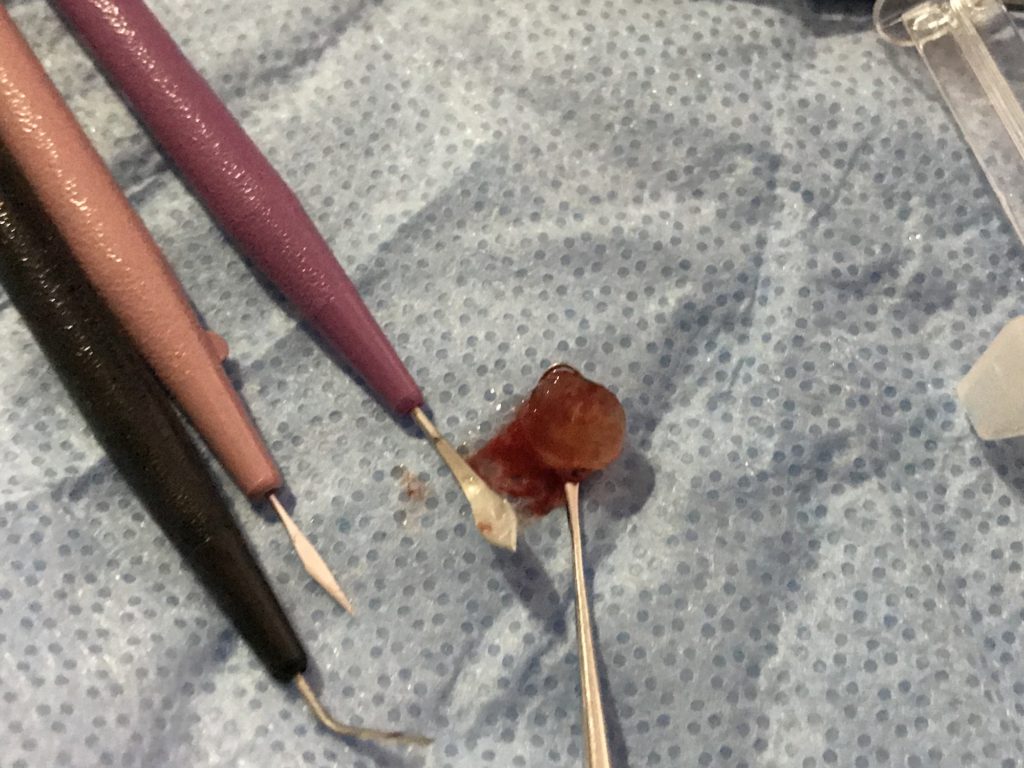
and just in case you want to see what a cataract looks like once it is removed out of the eye:
2:35 PM. We are taking a break for lunch
I eat plantain mashed for the first time.

After a short lunch break, we start on Andrew who traveled by bus for two days to come and get help from us.

We head over to the screening area to choose our next patient for surgery. Everybody want surgery done!
And the next patient is chosen!
The day continues on. More surgery. And here is our last patient of the day.

Before we leave the hospital to go back to the hotel, we made the round to check on our little four-year-old. He is doing just fine under the watchful eyes of his father.


Here is a look at the eye team screening room working in the dark, if you look carefully you will see a team member standing against the wall holding a flashlight so Dr. Major can write her notes after patient examination.
We did not get back to the hotel until 9 PM. The team went out to dinner, had fun. We are invited every night by some organization that would volunteer to pay for our dinner because they appreciate our work. However, we are too exhausted to go. The young people can go. We decided to just order some hotel food, eat, shower and sleep.
Give us your email address below and we will keep you updated on all new posts!